| Henry Gray (1821–1865). Anatomy of the Human Body. 1918. |
| |
| 3b. 3. The Urinary Bladder |
| |
(Vesica Urinaria; Bladder)
The urinary bladder (Fig. 1135) is a musculomembranous sac which acts as a reservoir for the urine; and as its size, position, and relations vary according to the amount of fluid it contains, it is necessary to study it as it appears (a) when empty, and (b) when distended.) In both conditions the position of the bladder varies with the condition of the rectum, being pushed upward and forward when the rectum is distended. | 1 |
| | | The Empty Bladder.—When hardened in situ, the empty bladder has the form of a flattened tetrahedron, with its vertex tilted forward. It presents a fundus, a vertex, a superior and an inferior surface. The fundus (Fig. 1152) is triangular in shape, and is directed downward and backward toward the rectum, from which it is separated by the rectovesical fascia, the vesiculæ seminales, and the terminal portions of the ductus deferentes. The vertex is directed forward toward the upper part of the symphysis pubis, and from it the middle umbilical ligament is continued upward on the back of the anterior abdominal wall to the umbilicus. The peritoneum is carried by it from the vertex of the bladder on to the abdominal wall to form the middle umbilical fold. The superior surface is triangular, bounded on either side by a lateral border which separates it from the inferior surface, and behind by a posterior border, represented by a line joining the two ureters, which intervenes between it and the fundus. The lateral borders extend from the ureters to the vertex, and from them the peritoneum is carried to the walls of the pelvis. On either side of the bladder the peritoneum shows a depression, named the paravesical fossa (Fig. 1037). The superior surface is directed upward, is covered by peritoneum, and is in relation with the sigmoid colon and some of the coils of the small intestine. When the bladder is empty and firmly contracted, this surface is convex and the lateral and posterior borders are rounded; whereas if the bladder be relaxed it is concave, and the interior of the viscus, as seen in a median sagittal section, presents the appearance of a V-shaped slit with a shorter posterior and a longer anterior limb—the apex of the V corresponding with the internal orifice of the urethra. The inferior surface is directed downward and is uncovered by peritoneum. It may be divided into a posterior or prostatic area and two infero-lateral surfaces. The prostatic area is somewhat triangular: it rests upon and is in direct continuity with the base of the prostate; and from it the urethra emerges. The infero-lateral portions of the inferior surface are directed downward and lateralward: in front, they are separated from the symphysis pubis by a mass of fatty tissue which is named the retropubic pad; behind, they are in contact with the fascia which covers the Levatores ani and Obturatores interni. | 2 |
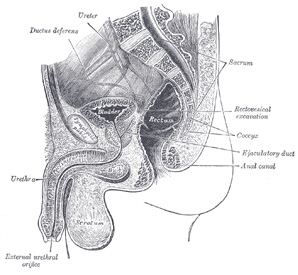 |
FIG. 1135– Median sagitta section of male pelvis. (See enlarged image) | | |
| When the bladder is empty it is placed entirely within the pelvis, below the level of the obliterated hypogastric arteries, and below the level of those portions of the ductus deferentes which are in contact with the lateral wall of the pelvis; after they cross the ureters the ductus deferentes come into contact with the fundus of the bladder. As the viscus fills, its fundus, being more or less fixed, is only slightly depressed; while its superior surface gradually rises into the abdominal cavity, carrying with it its peritoneal covering, and at the same time rounding off the posterior and lateral borders. | 3 |
| | | The Distended Bladder.—When the bladder is moderately full it contains about 0.5 liter and assumes an oval form; the long diameter of the oval measures about 12 cm. and is directed upward and forward. In this condition it presents a postero-superior, an antero-inferior, and two lateral surfaces, a fundus and a summit. The postero-superior surface is directed upward and backward, and is covered by peritoneum: behind, it is separated from the rectum by the rectovesical excavation, while its anterior part is in contact with the coils of the small intestine. The antero-inferior surface is devoid of peritoneum, and rests, below, against the pubic bones, above which it is in contact with the back of the anterior abdominal wall. The lower parts of the lateral surfaces are destitute of peritoneum, and are in contact with the lateral walls of the pelvis. The line of peritoneal reflection from the lateral surface is raised to the level of the obliterated hypogastric artery. The fundus undergoes little alteration in position, being only slightly lowered. It exhibits, however, a narrow triangular area, which is separated from the rectum merely by the rectovesical fascia. This area is bounded below by the prostate, above by the rectovesical fold of peritoneum, and laterally by the ductus deferentes. The ductus deferentes frequently come in contact with each other above the prostate, and under such circumstances the lower part of the triangular area is obliterated. The line of reflection of the peritoneum from the rectum to the bladder appears to undergo little or no change when the latter is distended; it is situated about 10 cm. from the anus. The summit is directed upward and forward above the point of attachment of the middle umbilical ligament, and hence the peritoneum which follows the ligament, forms a pouch of varying depth between the summit of the bladder, and the anterior abdominal wall. | 4 |
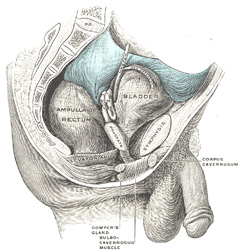 |
FIG. 1136– Male pelvic organs seen from right side. Bladder and rectum distended; relations of peritoneum to the bladder and rectum shown in blue. The arrow points to the rectovesical pouch. (See enlarged image) | | |
| | | The Bladder in the Child (Figs. 1137, 1138).—In the newborn child the internal urethral orifice is at the level of the upper border of the symphysis pubis; the bladder therefore lies relatively at a much higher level in the infant than in the adult. Its anterior surface “is in contact with about the lower two-thirds of that part of the abdominal wall which lies between the symphysis pubis and the umbilicus” (Symington 177). Its fundus is clothed with peritoneum as far as the level of the internal orifice of the urethra. Although the bladder of the infant is usually described as an abdominal organ, Symington has pointed out that only about one-half of it lies above the plane of the superior aperture of the pelvis. Disse maintains that the internal urethral orifice sinks rapidly during the first years, and then more slowly until the ninth year, after which it remains sta when it again slowly descends and reaches its adult position. | 5 |
 |
FIG. 1137– Sagittal section through the pelvis of a newly born male child. (See enlarged image) | | |
 |
FIG. 1138– Sagittal section through the pelvis of a newly born female child. (See enlarged image) | | |
| | | The Female Bladder (Fig. 1139).—In the female, the bladder is in relation behind with the uterus and the upper part of the vagina. It is separated from the anterior surface of the body of the uterus by the vesicouterine excavation, but below the level of this excavation it is connected to the front of the cervix uteri and the upper part of the anterior wall of the vagina by areolar tissue. When the bladder is empty the uterus rests upon its superior surface. The female bladder is said by some to be more capacious than that of the male, but probably the opposite is the case. | 6 |
 |
FIG. 1139– Median sagittal section of female pelvis. (See enlarged image) | | |
| | | Ligaments.—The bladder is connected to the pelvic wall by the fascia endopelvina. In front this fascial attachment is strengthened by a few muscular fibers, the Pubovesicales, which extend from the back of the pubic bones to the front of the bladder; behind, other muscular fibers run from the fundus of the bladder to the sides of the rectum, in the sacrogenital folds, and constitute the Rectovesicales. | 7 |
| The vertex of the bladder is joined to the umbilicus by the remains of the urachus which forms the middle umbilical ligament, a fibromuscular cord, broad at its attachment to the bladder but narrowing as it ascends. | 8 |
| From the superior surface of the bladder the peritoneum is carried off in a series of folds which are sometimes termed the false ligaments of the bladder. Anteriorly there are three folds: the middle umbilical fold on the middle umbilical ligament, and two lateral umbilical folds on the obliterated hypogastric arteries. The reflections of the peritoneum on to the side walls of the pelvis form the lateral false ligaments, while the sacrogenital folds constitute posterior false ligaments. | 9 |
| | | Interior of the Bladder (Fig. 1140).—The mucous membrane lining the bladder is, over the greater part of the viscus, loosely attached to the muscular coat, and appears wrinkled or folded when the bladder is contracted: in the distended condition of the bladder the folds are effaced. Over a small triangular area, termed the trigonum vesicæ, immediately above and behind the internal orifice of the urethra, the mucous membrane is firmly bound to the muscular coat, and is always smooth. The anterior angle of the trigonum vesicæ is formed by the internal orifice of the urethra: its postero-lateral angles by the orifices of the ureters. Stretching behind the latter openings is a slightly curved ridge, the torus uretericus, forming the base of the trigone and produced by an underlying bundle of non-striped muscular fibers. The lateral parts of this ridge extend beyond the openings of the ureters, and are named the plicæ uretericæ; they are produced by the terminal portions of the ureters as they traverse obliquely the bladder wall. When the bladder is illuminated the torus uretericus appears as a pale band and forms an important guide during the operation of introducing a catheter into the ureter. | 10 |
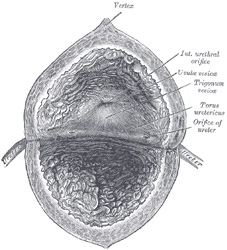 |
FIG. 1140– The interior of bladder. (See enlarged image) | | |
| The orifices of the ureters are placed at the postero-lateral angles of the trigonum vesicæ, and are usually slit-like in form. In the contracted bladder they are about 2.5 cm. apart and about the same distance from the internal urethral orifice; in the distended viscus these measurements may be increased to about 5 cm. | 11 |
| The internal urethral orifice is placed at the apex of the trigonum vesicæ, in the most dependent part of the bladder, and is usually somewhat crescentic in form; the mucous membrane immediately behind it presents a slight elevation, the uvula vesicæ, caused by the middle lobe of the prostate. | 12 |
| | | Structure (Fig. 1141).—The bladder is composed of the four coats: serous, muscular, submucous, and mucous coats. | 13 |
| The serous coat (tunica serosa) is a partial one, and is derived from the peritoneum. It invests the superior surface and the upper parts of the lateral surfaces, and is reflected from these on to the abdominal and pelvic walls. | 14 |
| The muscular coat (tunica muscularis) consists of three layers of unstriped muscular fibers: an external layer, composed of fibers having for the most part a longitudinal arrangement; a middle layer, in which the fibers are arranged, more or less, in a circular manner; and an internal layer, in which the fibers have a general longitudinal arrangement. | 15 |
| The fibers of the external layer arise from the posterior surface of the body of the pubis in both sexes (musculi pubovesicales), and in the male from the adjacent part of the prostate and its capsule. They pass, in a more or less longitudinal manner, up the inferior surface of the bladder, over its vertex, and then descend along its fundus to become attached to the prostate in the male, and to the front of the vagina in the female. At the sides of the bladder the fibers are arranged obliquely and intersect one another. This layer has been named the Detrusor urinæ muscle. | 16 |
| The fibers of the middle circular layer are very thinly and irregularly scattered on the body of the organ, and, although to some extent placed transversely to the long axis of the bladder, are for the most part arranged obliquely. Toward the lower part of the bladder, around the internal urethral orifice, they are disposed in a thick circular layer, forming the Sphincter vesicæ, which is continuous with the muscular fibers of the prostate. | 17 |
| The internal longitudinal layer is thin, and its fasciculi have a reticular arrangement, but with a tendency to assume for the most part a longitudinal direction. Two bands of oblique fibers, originating behind the orifices of the ureters, converge to the back part of the prostate, and are inserted by means of a fibrous process, into the middle lobe of that organ. They are the muscles of the ureters, described by Sir C. Bell, who supposed that during the contraction of the bladder they serve to retain the oblique direction of the ureters, and so prevent the reflux of the urine into them. | 18 |
| The submucous coat (tela submucosa) consists of a layer of areolar tissue, connecting together the muscular and mucous coats, and intimately united to the latter. | 19 |
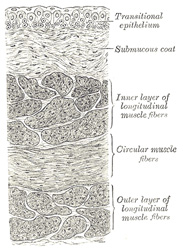 |
FIG. 1141– Vertical section of bladder wall. (See enlarged image) | | |
| The mucous coat (tunica mucosa) is thin, smooth, and of a pale rose color. It is continuous above through the ureters with the lining membrane of the renal tubules, and below with that of the urethra. The loose texture of the submucous layer allows the mucous coat to be thrown into folds or rugæ when the bladder is empty. Over the trigonum vesicæ the mucous membrane is closely attached to the muscular coat, and is not thrown into folds, but is smooth and flat. The epithelium covering it is of the transitional variety, consisting of a superficial layer of polyhedral flattened cells, each with one, two, or three nuclei; beneath these is a stratum of large club-shaped cells, with their narrow extremities directed downward and wedged in between smaller spindle-shaped cells, containing oval nuclei (Fig. 1141). The epithelium varies according as the bladder is distended or contracted. In the former condition the superficial cells are flattened and those of the other layers are shortened; in the latter they present the appearance described above. There are no true glands in the mucous membrane of the bladder, though certain mucous follicles which exist, especially near the neck of the bladder, have been regarded as such. | 20 |
| | | Vessels and Nerves.—The arteries supplying the bladder are the superior, middle, and inferior vesical, derived from the anterior trunk of the hypogastric. The obturator and inferior gluteal arteries also supply small visceral branches to the bladder, and in the female additional branches are derived from the uterine and vaginal arteries. | 21 |
| The veins form a complicated plexus on the inferior surface, and fundus near the prostate, and end in the hypogastric veins. | 22 |
| The lymphatics are described on page 712. | 23 |
| The nerves of the bladder are (1) fine medullated fibers from the third and fourth sacral nerves, and (2) non-medullated fibers from the hypogastric plexus. They are connected with ganglia in the outer and submucous coats and are finally distributed, all as non-medullated fibers, to the muscular layer and epithelial lining of the viscus. | 24 |
| | | Abnormalities.—A defect of development, in which the bladder is implicated, is known under the name of extroversion of the bladder. In this condition the lower part of the abdominal wall and the anterior wall of the bladder are wanting, so that the fundus of the bladder presents on the abdominal surface, and is pushed forward by the pressure of the viscera within the abdomen, forming a red vascular tumor on which the openings of the ureters are visible. The penis, except the glans, is rudimentary and is cleft on its dorsal surface, exposing the floor of the urethra, a condition known as epispadias. The pelvic bones are also arrested in development. | 25 |
|
|