| Henry Gray (1821–1865). Anatomy of the Human Body. 1918. |
| |
| 4c. Peculiarities in the Vascular System in the Fetus |
| |
| The chief peculiarities of the fetal heart are the direct communication between the atria through the foramen ovale, and the large size of the valve of the inferior vena cava. Among other peculiarities the following may be noted. (1) In early fetal life the heart lies immediately below the mandibular arch and is relatively large in size. As development proceeds it is gradually drawn within the thorax, but at first it lies in the middle line; toward the end of pregnancy it gradually becomes oblique in direction. (2) For a time the atrial portion exceeds the ventricular in size, and the walls of the ventricles are of equal thickness: toward the end of fetal life the ventricular portion becomes the larger and the wall of the left ventricle exceeds that of the right in thickness. (3) Its size is large as compared with that of the rest of the body, the proportion at the second month being 1 to 50, and at birth, 1 to 120, while in the adult the average is about 1 to 160. | 1 |
| The foramen ovale, situated at the lower part of the atrial septum, forms a free communication between the atria until the end of fetal life. A septum (septum secundum) grows down from the upper wall of the atrium to the right of the primary septum in which the foramen ovale is situated; shortly after birth it fuses with the primary septum and the foramen ovale is obliterated. | 2 |
| The valve of the inferior vena cava serves to direct the blood from that vessel through the foramen ovale into the left atrium. | 3 |
| The peculiarities in the arterial system of the fetus are the communication between the pulmonary artery and the aorta by means of the ductus arteriosus, and the continuation of the hypogastric arteries as the umbilical arteries to the placenta. | 4 |
| The ductus arteriosus is a short tube, about 1.25 cm. in length at birth, and of the diameter of a goose-quill. In the early condition it forms the continuation of the pulmonary artery, and opens into the aorta, just beyond the origin of the left subclavian artery; and so conducts the greater amount of the blood from the right ventricle into the aorta. When the branches of the pulmonary artery have become larger relatively to the ductus arteriosus, the latter is chiefly connected to the left pulmonary artery. | 5 |
| The hypogastric arteries run along the sides of the bladder and thence upward on the back of the anterior abdominal wall to the umbilicus; here they pass out of the abdomen and are continued as the umbilical arteries in the umbilical cord to the placenta. They convey the fetal blood to the placenta. | 6 |
| The peculiarities in the venous system of the fetus are the communications established between the placenta and the liver and portal vein, through the umbilical vein; and between the umbilical vein and the inferior vena cava through the ductus venosus. | 7 |
| | | Fetal Circulation (Fig. 502).—The fetal blood is returned from the placenta to the fetus by the umbilical vein. This vein enters the abdomen at the umbilicus, and passes upward along the free margin of the falciform ligament of the liver to the under surface of that organ, where it gives off two or three branches, one of large size to the left lobe, and others to the lobus quadratus and lobus caudatus. At the porta hepatis (transverse fissure of the liver) it divides into two branches: of these, the larger is joined by the portal vein, and enters the right lobe; the smaller is continued upward, under the name of the ductus venosus, and joins the inferior vena cava. The blood, therefore, which traverses the umbilical vein, passes to the inferior vena cava in three different ways. A considerable quantity circulates through the liver with the portal venous blood, before entering the inferior vena cava by the hepatic veins; some enters the liver directly, and is carried to the inferior cava by the hepatic veins; the remainder passes directly into the inferior vena cava through the ductus venosus. | 8 |
| In the inferior vena cava, the blood carried by the ductus venosus and hepatic veins becomes mixed with that returning from the lower extremities and abdominal wall. It enters the right atrium, and, guided by the valve of the inferior vena cava, passes through the formen ovale into the left atrium, where it mixes with a small quantity of blood returned from the lungs by the pulmonary veins. From the left atrium it passes into the left ventricle; and from the left ventricle into the aorta, by means of which it is distributed almost entirely to the head and upper extremities, a small quantity being probably carried into the descending aorta. From the head and upper extremities the blood is returned by the superior vena cava to the right atrium, where it mixes with a small portion of the blood from the inferior vena cava. From the right atrium it descends into the right ventricle, and thence passes into the pulmonary artery. The lungs of the fetus being inactive, only a small quantity of the blood of the pulmonary artery is distributed to them by the right and left pulmonary arteries, and returned by the pulmonary veins to the left atrium: the greater part passes through the ductus arteriosus into the aorta, where it mixes with a small quantity of the blood transmitted by the left ventricle into the aorta. Through this vessel it descends, and is in part distributed to the lower extremities and the viscera of the abdomen and pelvis, but the greater amount is conveyed by the umbilical arteries to the placenta. | 9 |
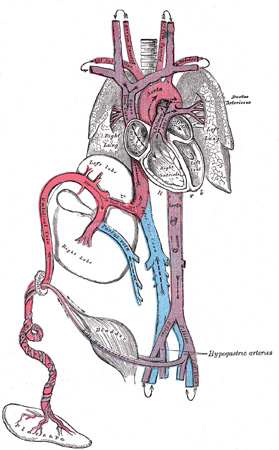 |
FIG. 502– Plan of the fetal circulation. In this plan the figured arrows represent the kind of blood, as well as the direction which it takes in the vessles. Thus—arterial blood is figured >—>; venous blood, >—>; mixed (arterial and venous) blood, >—>. (See enlarged image) | | |
| From the preceding account of the circulation of the blood in the fetus the following facts will be evident: (1) The placenta serves the purposes of nutrition and excretion, receiving the impure blood from the fetus, and returning it purified and charged with additional nutritive material. (2) Nearly the whole of the blood of the umbilical vein traverses the liver before entering the inferior vena cava; hence the large size of the liver, especially at an early period of fetal life. (3) The right atrium is the point of meeting of a double current, the blood in the inferior vena cava being guided by the valve of this vessel into the left atrium, while that in the superior vena cava descends into the right ventricle. At an early period of fetal life it is highly probable that the two streams are quite distinct; for the inferior vena cava opens almost directly into the left atrium, and the valve of the inferior vena cava would exclude the current from the right ventricle. At a later period, as the separation between the two atria becomes more distinct, it seems probable that some mixture of the two streams must take place. (4) The pure blood carried from the placenta to the fetus by the umbilical vein, mixed with the blood from the portal vein and inferior vena cava, passes almost directly to the arch of the aorta, and is distributed by the branches of that vessel to the head and upper extremities. (5) The blood contained in the descending aorta, chiefly derived from that which has already circulated through the head and limbs, together with a small quantity from the left ventricle, is distributed to the abdomen and lower extremities. | 10 |
| | | Changes in the Vascular System at Birth.—At birth, when respiration is established, an increased amount of blood from the pulmonary artery passes through the lungs, and the placental circulation is cut off. The foramen ovale is closed by about the tenth day after birth: the valvular fold above mentioned adheres to the margin of the foramen for the greater part of its circumference, but a slit-like opening is left between the two atria above, and this sometimes persists. | 11 |
| The ductus arteriosus begins to contract immediately after respiration is established, and is completely closed from the fourth to the tenth day; it ultimately degenerates into an impervious cord, the ligamentum arteriosum, which connects the left pulmonary artery to the arch of the aorta. | 12 |
| Of the hypogastric arteries, the parts extending from the sides of the bladder to the umbilicus become obliterated between the second and fifth days after birth, and project as fibrous cords, the lateral umbilical ligaments, toward the abdominal cavity, carrying on them folds of peritoneum. | 13 |
| The umbilical vein and ductus venosus are completely obliterated between the second and fifth days after birth; the former becomes the ligamentum teres, the latter the ligamentum venosum, of the liver. | 14 |
|
|